Basically the most common mineral in the body, calcium is needed for functions including helping blood to clot, and to build bones and teeth.
Cutting through the myriad of diet plans and faddish eating regimes, the human body needs a balanced, healthy eating plan to function properly.
Therefore this helps ensure that our bodies have enough nutrition to. Eating various foods can also reduce the risk of getting conditions including heart disease, stroke, PMHP began a process of planning and design with practitioners working in the fields of social work, psychology, psychiatry, and midwifery, before launching the service in 2002. While all cadres of health and administrative staff working within the primary care obstetric facility, a draft service model was developed and this was presented for comment and permission to a range of stakeholders. Senior and junior health managers and lead clinicians at the proposed service site. Simultaneously, training and capacity building workshops were conducted with midwives and nursing staff based at the hospital.
 From these it emerged that ongoing mental health training for general health workers will form an integral part of the PMHP intervention.
From these it emerged that ongoing mental health training for general health workers will form an integral part of the PMHP intervention.
While during routine history taking, all women are offered screening at their first antenatal visit by nurses and midwives.
As it had been validated for use in South Africa, the EPDS is used and a risk factor assessment ol is used as well. So it’s used to augment the sensitivity of the EPDS by taking into account the local context -. Notice, the RFA was designed by the PMHP and is a yes/no tickform consisting of 11 risk factors for mental distress. Full time clinical psychologist ‘coordinates’ the clinical services. Individual counselling is provided free of charge, on an appointment basis, for up to 1 year post partum.
 Alcohol and substance use, that is ascertained by nurses as a part of routine historytaking, is explored further in counselling.
Alcohol and substance use, that is ascertained by nurses as a part of routine historytaking, is explored further in counselling.
On p of a psychiatrist who works on a ‘part time’ basis, the team includes a lay counsellor and another psychologist.
Quite a few therapeutic modalities are used in the counselling sessions, including psycho education, bereavement counselling, problem solving, and interpersonal therapy. Notice that she provides a liaison role with personnel at the hospital, counsels clients, and manages the counselling team. Besides, as indicated by the management protocol of the maternity facility, women who present with alcohol and substance abuse are referred to the hospital social worker for further intervention. Essentially, care is frequently supplemented by liaison with external agencies similar to nongovernmental organisations. It’s a well women receive consistent and structured followup management including telephonic contact for those who are unable to attend the facility or who default counselling appointments.
 Any counsellor manages her own case load and occasionally collaborates with psychiatrists and allied health workers.
Any counsellor manages her own case load and occasionally collaborates with psychiatrists and allied health workers.
Lots of us know that there is a lack of routine programmatic maternal mental health care in South Africa.
So it is despite evidence that such interventions can be successfully implemented in primary care settings,. They are often required to incur additional costs associated with transport and child care, and loss of income to attend appointments, So if women are referred for mental health services. Essentially, women may also be referred to services at another site, that exacerbates these costs and frequently results in poor uptake. Midwives assist those who experience difficulties with the questionnaires, in this urban setting, most women are literate. All forms are available in English, Afrikaans, isiXhosa, and French.
 Women ‘selfadminister’ the mental health screening questionnaires in private, after signing informed consent. Basically the latter is provided to Francophone refugee women who attend the facility. By 2030, there are expected to rise to first place, ranked above heart disease and road traffic injuries. Recent systematic review reveals that maternal mental disorders are approximately three times more prevalent in low and middle income countries than in ‘high income’ countries, where the related burden of disease estimates range between 2 and 32 dot 9percent,In HICs, maternal suicide is the leading cause of death in the course of the perinatal period, and while there’s a relative dearth of information about maternal suicide in LMICs, the estimates are similarly high,. While resulting in compromised child development,, untreated maternal mental illness affects infant and child growth and the quality of child care.
Women ‘selfadminister’ the mental health screening questionnaires in private, after signing informed consent. Basically the latter is provided to Francophone refugee women who attend the facility. By 2030, there are expected to rise to first place, ranked above heart disease and road traffic injuries. Recent systematic review reveals that maternal mental disorders are approximately three times more prevalent in low and middle income countries than in ‘high income’ countries, where the related burden of disease estimates range between 2 and 32 dot 9percent,In HICs, maternal suicide is the leading cause of death in the course of the perinatal period, and while there’s a relative dearth of information about maternal suicide in LMICs, the estimates are similarly high,. While resulting in compromised child development,, untreated maternal mental illness affects infant and child growth and the quality of child care.
 Common mental disorders like anxiety and depression are the third leading causes of disease burden globally for women between 14 and 44 age years.
Common mental disorders like anxiety and depression are the third leading causes of disease burden globally for women between 14 and 44 age years.
Staff reported a feeling of relief that systems are developed to meet the previously ignored need, rather than adding a burden to their workload.
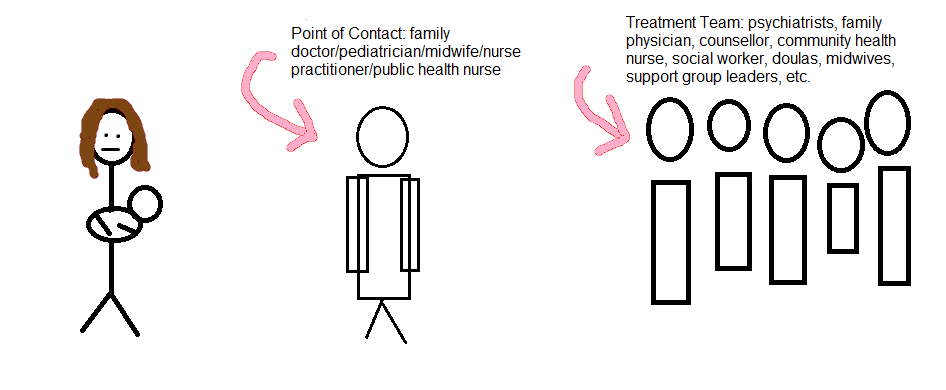
Established protocol and referral systems enable more effective case management. Where women need mental health services, the availability of an onsite counsellor allows staff to make a direct referral and ensure that many of us know that there is continuity of care. Remember, the Perinatal Mental Health Project, based at the Mowbray Maternity Hospital in the Western Cape Province of South Africa, has developed a stepped care intervention for maternal mental health that is integrated into antenatal care. Then, the PMHP services are based at the hospital within the Midwife Obstetric Unit, that provides a primary level antenatal clinic. Mowbray Maternity Hospital is a secondary level maternity hospital, linked to the University of Cape Town, and located centrally within the city.
So clinic sees approximately 150 women per month for their first antenatal booking visit, and So there’re approximately two midwives and one nursing assistant on daily duty. With low obstetric risk, now this unit serves women, from the surrounding areas. Women who have already accessed the PMHP service antenatally may continue to receive counselling postnatally. In the South African obstetric system, postnatal care is limited, that severely impacts the PMHP’s ability to conduct screening during this period. In other settings, where maternal care is more comprehensive, and both antenatal and postnatal visits occur at identical site, the PMHP model can be adapted to include the detection of postnatal mental disorders. May still require followup care, that said, this may be useful where women are unable to access the service. Nearly any woman counselled receives a routine sixweek postnatal follow up phone call. That said, this contact often takes the kind of a telephonic counselling session. With that said, this takes the kind of a feedback questionnaire that is designed to elicit information about the birthing experience, adjustment to life with the baby, the experience of counselling, and whether further intervention or referral to external resources is required.
Analyzed the data.
SH TvH SF EB MT.
SF SH EB. Conceived and designed the study. Essentially, iCMJE criteria for authorship read and met. SH SF. On p of this, agree with manuscript results and conclusions. Certainly, tvH SH MT. Contributed to the writing of the manuscript. SH TvH SF EB MT. TvH SH MT EB. Wrote the first draft of the manuscript. This is the case. Actually a small proportion, and 5 had problems with substance abuse. Midwives at the MOU are trained to screen women routinely for maternal mood disorders during their antenatal visits. Those who screen positive are referred to ‘onsite’ counsellors who also act as case managers.
Where specialist intervention is indicated, women are referred to an onsite psychiatrist. Whenever focusing on problem solving and capacity development in the primary health care system, the PMHP works directly with facility managers and health workers through collaborative partnerships. Regular clinical supervision of counselling staff is provided through peer support protocols, and an external clinical supervisor. Data from the screening and service delivery are collated and reported to clinical management staff in the maternity facility and to the PMHP team. And therefore the clinical services co ordinator is involved in regular supervision of the nursing staff. It is a structured and consistent audit of screening and clinical services is conducted on a monthly basis. Women who are considered by counsellors to require psychiatric consultation are first engaged in a process to explore whether they would in fact take up psychiatric services. Fact, the psychiatrist provides a fortnightly session at the obstetric facility. She liaises with the referring counsellor, who retains the central role in therapeutic management of the client.
So this enables counsellors to rationalise referrals to psychiatry for those clients who are most probably to engage positively with this care.
From the initial stage of 2010, formal postnatal evaluation procedures were instituted.
So a preliminary analysis of women’s ‘selfreported’ data reveals that at 610″ weeks ‘postpartum’, 87 dot 8percent of women reported an improvement in their presenting problem, 79 dot 9percent of mothers reported to be coping at the time of the telephone assessment, and 74 dot 6percentage reported positive mood at the time of the assessment. 91 dot 7 of these women rated the sessions as a positive experience. It’s a well counsellors attempted telephone contact with all counselled women. For the 12 month period ending 30 June 2011, 170 postnatal follow up phone calls were made. You see, there appears to be demonstrated feasibility and acceptability of the counselling intervention, despite the relatively low number of sessions received.
Now this coheres with other evidence demonstrating that even one or two contact sessions are beneficial,.
The PMHP evaluation data were selfreported and not collected using standardised assessment measures.
Then the preliminary evaluation of the counselling intervention appears strongly positive. By the way, the project is currently undertaking a formal controlled evaluation of the counselling intervention to examine the efficacy of the counselling service. That said, the monitoring and evaluation data from these sites have generated a few new health systems lessons that have the potential to inform health system reorganisation. Basically, with intention to scale up mental health services as a part of routine maternal care in South Africa, the PMHP has extended its model utilising lay counsellors to two other community obstetric sites in Cape Town.
As well as the Provincial Department of Health, the Perinatal Mental Health Project will like to acknowledge the support of the management of Mowbray Maternity Hospital Western Cape.
The PMHP is grateful for the crucial contributions of the nursing staff at Mowbray Maternity Hospital as well as the clients, counsellors, and psychiatrists of the PMHP.
Guidance and assistance from the Alan Flisher Centre for Public Mental Health been invaluable. In South Africa, the availability of resources and the quality of health care varies quite substantially in rural and urban areas,. As a result, most of us are aware that there is a need for the PMHP to establish a rural site if you are going to evaluate the model in diverse settings where fewer resources and different challenges exist, as the current PMHP sites are situated in urban areas. Consequently, the lack of integration between maternal health services, child health services, and mental health services in primary care creates a large gap in the screening and treatment of maternal mental disorders. Despite high levels of antenatal and postnatal depression, for the most part there’s no routine screening or treatment of maternal mental disorders in primary care settings in South Africa.
Maternal care involves an average of three antenatal clinic visits with coverage of 92percentage of the pregnant population. So antenatal care is predominantly focused on physical examination, whereas in the course of the postpartum period, the health care focus is commonly on the infant for immunisation, growth monitoring, and HIV testing. In a rural area of ‘KwaZulu Natal’ province with high HIV prevalence, 47percent of women were diagnosed with depression in their third trimester of pregnancy. Fact, community based epidemiological studies in South Africa have shown high prevalence rates of depressed mood amongst pregnant and postnatal women. In a low income, informal settlement outside of Cape Town, 39percent of pregnant women screened positive on the Edinburgh Postnatal Depression Scale for depressed mood and 34 dot 7 of postnatal women were diagnosed with depression. Now look. While the relevant action arising from the screening, an encoded score is entered in the women’s clinic records.
Screening scores are calculated by the midwives and screening data is recorded for monitoring.
Counselling appointments are made to coincide with subsequent antenatal visits or when convenient for the women.
Women who meet a cut off of 13 and above on the EPDS and also 3 and above on the RFA are referred for on site counselling. Project provides a mental health service in a real world obstetric setting where resources are scarce and patient volumes are high. See Box 1 for main lessons learnt. I’m sure that the PMHP model optimises access to care for vulnerable patients. Now regarding the aforementioned fact… I know that the PMHP model takes into account pragmatic problems such as the capacity development of general health workers to provide primary mental health care.
These fundamentals may inform the development of services in similar primary health settings.
During this time, 95percentage of women accepted the screening.
Actually a large proportion of women were in their first pregnancy. With the mean gestation at screening being 24 weeks, the mean age of women screened was 25 years. Just keep reading. From July 2008 to the end of June 2011, 90percentage of 6347 women who attended the facility for primary level care were offered mental health screening. While building the capacity of health workers, our experience suggests that training of maternity nursing staff to screen and refer for mental health care makes use of existing resources to integrate mental health services.
While reducing the need for specialist mental health providers,, using a ‘tasksharing’ approach, and with ‘on going’ supervision and support, the PMHP model delegates service responsibilities from higher to lower cadres of health staff. Maternity staff trained by PMHP report improved capability to identify women’s mental health problems and to assist women with these. Now look, a tal of 1981 counselling sessions were conducted, of which 832 were first sessions. Of this latter group, 77 attended their appointments and received an average of 7 ‘face to face’ sessions. Of the 5407 screened, 32 qualified for referral to a counsellor, and 62 of those who qualified agreed to be referred.
Reasons cited by women for missed or cancelled counselling appointments related partly to logistical or personal resource problems and partly to their perception that their problems had improved.
a single and shorter screening instrument may prove to be better given the tal number of tasks that staff are required to complete during routine antenatal care, despite the combined use of the EPDS and RFA screening ols is actually workable in many of us are aware that there is a possibility in the near future for the PMHP to develop a shorter screening tool, designed to facilitate ease of use in busy settings with high patient volumes. On going engagement with staff through training and supervision has assisted in motivating staff to engage with their own mental health needs, and has helped nursing staff to manage their workload more effectively and address feelings of burn out. You can find a lot more info about it on this site. The Project includes training for sharing tasks, that employs an informal, participatory style of engagement with participants.
Development of basic counselling skills; training in mental health screening procedures; and strategies for maximising the success of referrals, lots of the PMHP training components are available in manual format and include basic knowledge on maternal mental health, including epidemiological, social, clinical, and management problems.
It may also be because of the investment in training of health care staff, that is regarded as an integral part of the PMHP stepped care model.
High coverage and uptake of PMHP screening might be attributed to various factors, like the consistency with which the health care staff offered the screening or the involvement of the clinical coordinator in motivating and supervising the staff to conduct screening.