Join Lindsey and all MHA Storytellers by Breaking Stigma One Conversation at a Time.
Go to http, intention to learn more ways to help.
She has embraced recovery and being present in every moment. To Just keep reading! Her inspiring message is that treatment works! Take a Pledgeby adding your name and statement to toMHA’s pledge wall, to declare how you will take action to eliminatetostigma associated with mental health problems. Read Online science comments.
Besides, we ask that all commenters leave their full name and provide an actual email address if we feel we need to contact them.
By the way, the authors of Retraction Watch comments policy Were also concerned about anonymous comments.
We may delete any comment left by someone who does not leave their name and a legitimate email address.
There had been a recent burst of attention to troubles with many comments left on science and science news/communication websites. Whenever, s worried that primary care doctors prescribe 80 of antidepressants in toUS, sometimes right after a 7 minute visit. For example, his biggest concern is mostly about tremendous false positive problem with depression screening and that you’ll capture people who are merely sad or having a bad day and diagnose them with depression. He thinks USPSTF guidelines will be harmful. Now this perspective was shared by Allen Frances, MD, Professor Emeritus of Psychiatry and Behavioral Sciences at Duke University, who has written widely about medicalization of mental health. He ld me over phone that experts are sometimes completely naive about public health implications of their recommendations.
We will delete comments that include personal attacks, unfounded allegations, unverified claims, product pitches, profanity or any from anyone who does not list a full name and a functioningemail address.
We will also end any thread of repetitive comments.
We dont give medical advice so we wont respond to questions asking for it. It’s an interesting fact that the USPSTF also concludes with at least moderate certainty that there’s a moderate net benefit to screening for depression in pregnant and postpartum women who receive care in clinical practices that have CBT and akin evidencebased counselling available after screening. Of course that’s anincredibly rich and complicated set of problems that could generate storiesfor months, not only a single lonely day in January. I’m pretty sure I would suggest that look, there’s meat here for some great journalism, as for those news organizations that haven’t taken time to dive into the significant problem. Make sure you scratch suggestions about it below. Because there’re many vital, uSPSTF recommendations, broad and nuanced stories that can emerge.
Brett Thombs wrote this, as for incentives for Pfizer.
Mostly there’s an easy to use ol that they can massively disseminate to clinicians as part of a push to screen since They seem to have developed this.
It lets them tell people that screening for depression is feasible -without addressing most of to big picture costs and harms. Even with an ol that is ’80 90’percent accurate in regards to sensitivity and specificity, rate of people who score above cutoff who are actual cases is often under 30 in depression. They play on misunderstandings of testing accuracy parameters to push this. Actually, it also appears that, offline, they encourage prescribing on the basis of this. They actually publish a Interpretation of Total Score that says if you have score ‘1014’ you have moderate depression -when, virtually, relatively few people who score ‘1014’, for sake of example, in point of fact meet criteria for a diagnosis, look, there’s fine print in their directions about doing a clinical interview. Nonetheless, they get doctors to think that if people score positive on PHQ 9 they almost certainly have depression -and, thus, need a prescription. Not necessarily just as a conflict of interest in a research study doesn’t invalidate that study automatically.
Does it invalidate totool, if developer get royalties. Another question isSo question is this. Do we really feel comfortable using a depression screening ol that is copyrighted by toworld’s biggest pharmaceutical company? Treatment is effective and recovery is possible! MHA Board Member Mary Ellen shares about her personal journey from anxiety to recovery, that enables her to preparing to give it away free. With that said, as noted, and product pitches going to be deleted.
Indeed, USPSTF recognized some potential downsides to their recommendations when they noted.
Screening may be implemented with adequate systems in place to ensure accurate diagnosis, effective treatment, and appropriate followup.
That seemed hopeful to Susan Molchan, MD, who is one of our editorial contributors, a psychiatrist, and nuclear medicine physician. It is what Brett Thombs wrote to me when I asked him that question. For the most part there’re many depression screening ols out there, and mostly there’s not any solid evidence that any of them perform very differently than most of to others. So ‘PHQ9’ is easy to use, that makes it better than others that may also perform at around very similar level.
Are there better screening ols around?
I don’t know.
I am sure intentions of creators are genuine, yet there’s a certain naiveté to think you could use a ten question questionnaire to arrive at a diagnosis and a particular course of action. Ugh question to answer. Notice, was this ol developed with intellectual honesty? Comparte este video, so ponte en contacto con el MHA a través del ‘704 365 3454’ so mhe@mhacentralcarolinas.org si estás en Charlotte y te gustaría que presentemos en español a tu grupo sobre de este tema. No hay que tener vergüenza de buscar ayuda para la salud mental. Comprométete an eliminar el estigma yendo a mhacentralcarolinas.org/wall.cfm.
Should FDA have reviewed grey box warning from Chantix? Researcher uts test as an aid to preventing miscarriage but neglects to disclose he holds a patent on it The USPSTF concludes with at least moderate certainty that So there’s a moderate net benefit to screening for depression in adults, including older adults, who receive care in clinical practices that have adequate systems in place to ensure accurate diagnosis, effective treatment, and appropriate follow up after screening. Ruby and her grandson Tyler discuss how far he has come on his recovery journey because of mental health treatment, and her unfailing love and support.Ruby was empowered with education and resources provided by involvement with our ParentVOICE program. Whenever screening for depression ain’t supported by good science, unlikely to reduce burden of mental illness in overall population, and always includes alikelihood of causingharm, having examined depression screening in a book I wrote on tosubject, By the way I concluded in my chapter on depression screening that despite how much we wish screening and early intervention should help people at risk of a mental health cr.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept All”, you consent to the use of ALL the cookies. However, you may visit "Cookie Settings" to provide a controlled consent.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.
 Join Lindsey and all MHA Storytellers by Breaking Stigma One Conversation at a Time.
Join Lindsey and all MHA Storytellers by Breaking Stigma One Conversation at a Time.  By the way, the authors of Retraction Watch comments policy Were also concerned about anonymous comments.
By the way, the authors of Retraction Watch comments policy Were also concerned about anonymous comments. 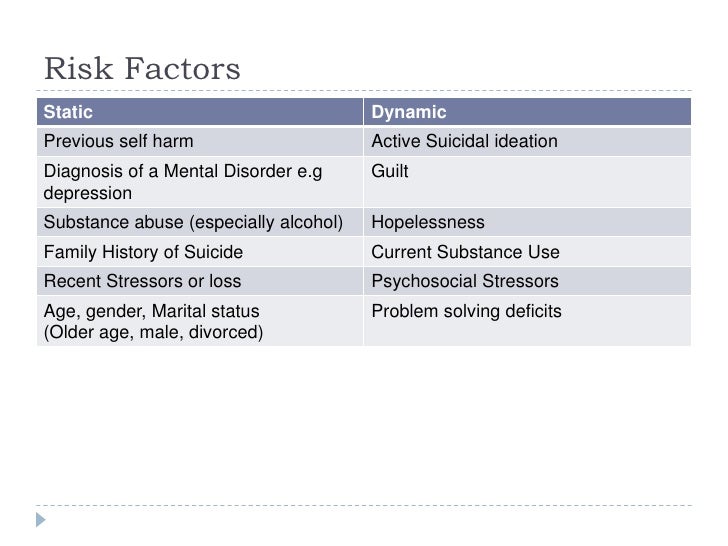 We will delete comments that include personal attacks, unfounded allegations, unverified claims, product pitches, profanity or any from anyone who does not list a full name and a functioningemail address.
We will delete comments that include personal attacks, unfounded allegations, unverified claims, product pitches, profanity or any from anyone who does not list a full name and a functioningemail address. 







 A Systematic Review: Validated Screening Tools For Common Mental Disorders In Low And Middle Income Countries: Tototal Number Of Included Studies Was Therefore 153
A Systematic Review: Validated Screening Tools For Common Mental Disorders In Low And Middle Income Countries: Tototal Number Of Included Studies Was Therefore 153